

Urinary
tract infection (UTI)
What is the urinary
tract?
The
urinary tract makes and stores pee. It includes:
·
Kidney
·
Ureters
·
Bladder
·
Urethra
1.
The kidneys are two bean-shaped organs that filter your
blood. Kidneys are small, bean-shaped
organs on the back of your body, above your hips. Most people have two kidneys.
They filter water and waste products from your blood, which becomes pee. Common
wastes include urea and creatinine.
Your kidneys filter about 200 quarts of fluid every day —
enough to fill a large bathtub. During this process, your kidneys remove waste,
which leaves your body as urine (pee). Most people pee about two quarts daily.
Your body re-uses the other 198 quarts of fluid.
Your kidneys also help balance your body’s fluids (mostly
water) and electrolytes. Electrolytes are essential minerals that include
sodium and potassium.
2.
What is a uterus?

Your uterus is a
pear-shaped organ in the reproductive system of people assigned
female at birth (AFAB). It’s where a fertilized egg implants during pregnancy
and where your baby develops until birth. It’s also responsible for your
menstrual cycle.
What does a uterus do?
Your uterus plays a
key role in your reproductive health and function. The three main jobs of your
uterus are:
- Pregnancy: Your uterus
stretches to grow your baby during pregnancy. It can also contract to help
push your baby out of your vagina.
- Fertility: Your uterus
is where a fertilized egg implants during conception and where
your baby grows.
- Menstrual cycle: Your
uterine lining is where blood and tissue come from during menstruation.
3.
Urethra
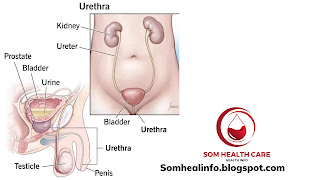
The urethra is the tube that lets
urine leave your bladder and your body. If you were assigned male at birth,
your urethra passes through your prostate and into your penis. If you were
assigned female at birth, your urethra is much shorter. It runs from your
bladder to open in front of your vagina.
What does the urethra do?
The urethra is part
of your urinary system. This system is made up of your kidneys, bladder,
ureters and urethra. Your kidneys clean your blood and produce urine, a waste
product. From your two kidneys, two ureters move the urine to the bladder,
where it’s stored until you urinate (pee). Urine leaves your body through a
hole at the end of your urethra. That hole from the inside to the outside is
called the urethral meatus. (The term ‘meatus’ refers to any opening from the
inside to the outside.
A urinary tract infection (UTI) is an infection in any part of the
urinary system. The urinary system includes the kidneys, ureters, bladder and
urethra. Most infections involve the lower urinary tract — the bladder and the
urethra.
Women are at greater risk of developing a UTI than are men. If
an infection is limited to the bladder, it can be painful and annoying. But
serious health problems can result if a UTI spreads to the kidneys.
Health care providers often treat urinary tract infections with
antibiotics. You can also take steps to lower the chance of getting
a UTI in the first place.
Urinary
tract infections (UTIs) are one of the most frequent clinical bacterial
infections in women, accounting for nearly 25% of all infections. Around 50–60%
of women will develop UTIs in their lifetimes. Escherichia coli is
the organism that causes UTIs in most patients. Recurrent UTIs (RUTI) are
mainly caused by reinfection by the same pathogen. Having frequent sexual
intercourse is one of the greatest risk factors for RUTIs. In a subgroup of
individuals with coexisting morbid conditions, complicated RUTIs can lead to
upper tract infections or urosepsis. Although the initial treatment is
antimicrobial therapy, use of different prophylactic regimens and alternative
strategies are available to reduce exposure to antibiotics.
Classification of UTI
UTIs
are classified into six categories.
The
first category is an uncomplicated infection; this is when
the urinary tract is normal, both structurally and physiologically, and there
is no associated disorder that impairs the host defense mechanisms.
The second category is a complicated
infection; this is when infection occurs within an abnormal urinary tract,
such as when there is ureteric obstruction, renal calculi, or vesicoureteric
reflux.
The third category, an isolated
infection, is when it is the first episode of UTI, or the episodes are 6
months apart. Isolated infections affect 25–40% of young females.
The fourth category, an unresolved
infection, is when therapy fails because of bacterial resistance or due to
infection by two different bacteria with equally limited susceptibilities.
The fifth category, reinfection,
occurs where there has been no growth after a treated infection, but then the
same organism regrows two weeks after therapy, or when a different
microorganism grows during any period of time.
The sixth category, relapse, is
when the same microorganism causes a UTI within two weeks of therapy; however,
it is usually difficult to distinguish a reinfection from a relapse.
Clinical Diagnosis
Common
symptoms of a UTI are dysuria, urinary frequency, urgency, suprapubic pain and
possible haematuria. Systemic symptoms are usually slight or absent. The urine
may have an unpleasant odour and appear cloudy
Diagnosis
of RUTI depends on the characteristic of clinical features, past history, three
positive urinary cultures within the previous 12-month period in symptomatic
patients and the presence of neutrophils in the urine (pyuria).
The
probability of finding a positive culture in the presence of the above symptoms
and the absence of vaginal discharge is around 81%.
In a
complicated UTI, such as pyelonephritis, the symptoms of a lower UTI will
persist for more than a week with systemic symptoms of persistent fever,
chills, nausea and vomiting.
The
presence of irritative voiding symptoms between perceived episodes of UTI
suggests a non-infectious cause as seen in interstitial cystitis, urethral
syndrome or detrusor muscle over activity.
General therapy and consultancy
Patients should be advised and encouraged to drink plenty
of fluids (two to three litters per day) and to urinate frequently to help
flush bacteria from the bladder. Holding urine for a long time allows bacteria
to multiply within the urinary tract, resulting in cystitis. Preventive measures
related to sexual intercourse may reduce the recurrence rate. Moreover, women
are encouraged to clean the genital areas before and after sex and to wipe from
front to back, which will reduce the spread of E. coli from the
perigenital area to the urethra.
Avoiding multiple sexual partners will reduce the risk of
both UTIs and sexually transmitted infections. Women are encouraged to avoid
spermicidal contraceptives, diaphragms and vaginal douching, which may irritate
the vagina and urethra and facilitate the entry and colonization of bacteria
within the urinary tract. Skin allergens introduced to the genital area, such
as bubble bath liquids, bath oils, vaginal creams and lotions, deodorant sprays
or soaps are better avoided as they could alter vaginal flora and ultimately
result in UTIs.
Antimicrobial
therapy
Antimicrobial therapy is the core treatment for UTIs,
with the main objective being the eradication of bacteria growth in the urinary
tract through an efficacious, safe and cost-effective antimicrobial agent. This
can be achieved within hours if the antibiotics are maintained at sufficient
urine levels. In order to ensure compliance and be patient-friendly, the
drug should be given for a short period of time to prevent bacterial
resistance. Antimicrobial agents should be prescribed according to the
susceptibility of the infecting bacteria, the concentrations of uropathogens in
the urine and the urinary complaint. This is important to consider when there
is septicaemia or parenchymal infection, as antimicrobials are usually at
higher levels in the urine than in serum.
Dose modification is required for
patients with renal insufficiency and in the case of other factors such as:
age, pregnancy or lactation status, primary or recurrent infections, hospitalized
patients, DM, liver disease, an immune compromised state, hydration levels and
psychiatric problems.
Ampicillin,
amoxicillin, and sulfonamides are no longer the drugs of choice for empirical
treatment because of the widespread emergence of resistance in 15–20% of E.
coli in several areas of the USA and other countries. Nitrofurantoin
or amoxicillin/clavulanic acid remain effective in terms of bacterial
sensitivity, but nitrofurantoin needs to be avoided in patients with
pyelonephritis because of its poor serum and tissue levels. Less than 5%
of E. coli strains are resistant to nitrofurantoin, whereas
other strains are often resistant to it. Penicillin’s and cephalosporin’s are
considered safe during pregnancy, but trimethoprim, sulphonamides, and fluoroquinolones
should be avoided. Oral antibiotic therapy resolves 94% of uncomplicated UTIs,
although recurrence is not uncommon. In the recently published International
Clinical Practice Guidelines for the Treatment of Acute Cystitis, a 3-day
regimen of trimethoprim-sulfamethoxazole (TMP-SMX) and a 5-day course of
nitrofurantoin are recommended as a first-line therapy for the management of
uncomplicated UTIs. A 5-day course of nitrofurantoin has an efficacy equivalent
to a 3-day TMP-SMX course.
3-
to 7-days regimen of beta-lactams, such as cefaclor or amoxicillin/clavulanic
acid, is appropriate when first-line therapies cannot be used. Although a 3-day
course of fluoroquinolones can be quite effective, it is not usually
recommended as first-line therapy because of the emerging resistance to them
and their potential side effects, as well as the high cost; nevertheless,
fluoroquinolones are the drug of choice in women who are experiencing low
tolerance or an allergic reaction after empirical therapy.
In a
meta-analysis, a single-dose regimen of fosfomycin trometamol has been shown to
be a safe and effective alternative for the treatment of UTIs in both pregnant
and non-pregnant women, as well as in elderly and paediatric patients, but it
seems to be slightly less effective than the above mentioned therapies. Pivmecillinam
in a 3- to 7-day course is also effective, but not available in most regions.
Because of its poor efficacy, amoxicillin and ampicillin should not be used for
the empirical treatment of UTIs.
ACUTE SELF-TREATMENT
The patient self-treatment management strategy is an
ideal effort to decrease overall antibiotic consumption, and for women who are
not suitable candidates for long-term daily prophylaxis. Schaeffer showed that
“self-start therapy” should be confined to those women who are self-motivated
and have good compliance. A patient needs to consult a physician
immediately if she becomes pregnant or if there is any change in symptoms, an
increased recurrence of episodes of infection, or no change in symptoms within
48 hours of antimicrobial treatment. These patients can effectively self-treat
RUTIs by initiating a standard 3 day course of recommended antimicrobials with
minimum side effects.




){kind=link}
0 Comments